Bpc 157 Diverticulitis Multifunctionality and Possible Medical Application of the BPC 157 Peptide—Literature and Patent Review
When “gut healing” claims meet real medicine, what actually holds up?
If you’ve ever sifted through research on peptides and thought, “Okay, but does this translate to something like diverticulitis?”—you’re not alone. In my hands-on work reviewing biomedical literature for translational plausibility, I’ve learned that the hardest part isn’t finding activity signals; it’s separating mechanistic rationale, formulation/route constraints, and patent-covered claims from the evidence that would actually support clinical use.
This article reviews bpc 157 diverticulitis from a “what the literature and patents collectively suggest” angle: multifunctionality (how the peptide is proposed to work across tissues), possible relevance to inflammatory bowel conditions, and the practical limitations you should understand before drawing conclusions.
What BPC 157 is (and why it’s often discussed as a “multifunctional” peptide)
BPC 157 is a peptide frequently discussed in experimental settings for its reported ability to influence processes involved in healing and tissue protection. When people call it “multifunctional,” they’re usually referring to the observation that it’s been investigated across multiple organ systems and endpoints—such as:
- Tissue repair and protection (e.g., wound-healing–type endpoints in preclinical models)
- Inflammation modulation (signals suggesting a reduction in inflammatory activity)
- Angiogenesis and microcirculation–related pathways (in some experimental contexts)
- Gastrointestinal resilience (studies that emphasize protection of the GI tract under stressors)
In my reviews, the “multifunctional” label is best understood as a pattern in preclinical endpoints rather than proof of a single, specific clinical mechanism. The logic typically looks like this:
- If a compound influences pathways tied to inflammation and tissue integrity, then it may be plausibly beneficial in conditions where those pathways are dysregulated.
- If a compound shows GI-tract protection in models, then it becomes a candidate for hypotheses about gut inflammatory diseases.
That hypothesis—gastrointestinal protection + anti-inflammatory influence—is where interest in bpc 157 diverticulitis discussions originates.
Why diverticulitis is a specific and challenging target for peptide claims
Diverticulitis isn’t just “inflammation of the gut.” Clinically, it involves:
- Localized inflammation and possible infection within colonic diverticula
- A spectrum from uncomplicated disease to complications (abscess, perforation, fistula)
- Often a time-sensitive decision framework (antibiotics, supportive care, drainage/surgery when needed)
So when someone claims a peptide could “treat” diverticulitis, the translational bar is high. In real-world terms, the question is not whether tissue pathways can be affected; it’s whether the intervention can:
- Reduce disease progression in humans
- Support resolution without masking worsening infection
- Achieve adequate exposure at the relevant site (local availability in the colon, appropriate pharmacokinetics)
- Demonstrate safety in the clinical context of acute GI inflammation
In my hands-on experience reviewing translational gaps, these are where many promising preclinical compounds lose credibility: endpoints can look encouraging, but human disease complexity introduces barriers such as heterogeneous disease mechanisms and different exposure/route dynamics.
Literature and patent patterns: what the evidence tends to emphasize
From a combined literature-and-patent perspective, BPC 157 is often framed as a candidate for protecting tissue integrity under stress, with proposed relevance to the GI tract. In practical terms, the most consistent themes you’ll see across documents are:
- Tissue-protective framing rather than a single disease-specific claim
- Cross-system endpoints that motivate “multifunctionality” (not necessarily diverticulitis-specific)
- Mechanistic storytelling that connects inflammation reduction and repair processes
How this relates to “bpc 157 diverticulitis” interest
When researchers or marketers connect BPC 157 to diverticulitis discussions, the usual reasoning is indirect:
- Diverticulitis involves inflammation and tissue injury.
- BPC 157 research often includes signals related to inflammation modulation and tissue repair.
- Therefore, BPC 157 might help the gut recover from inflammatory injury.
That’s a plausible hypothesis, but it’s not the same as evidence of clinical benefit in diverticulitis patients. If you want to evaluate credibility, I recommend looking for:
- Disease-model specificity: studies that resemble diverticulitis pathophysiology more closely than generic colitis models
- Clinically relevant outcomes: resolution metrics, complications, and safety signals—not only molecular markers
- Exposure/route alignment: whether the route used in preclinical work plausibly matches what would be used clinically
In my earlier audits of translational proposals, I’ve found that “GI protection” claims can be real, yet still fail the diverticulitis-specific test due to differences between colitis-like inflammation and diverticula-centered disease progression.
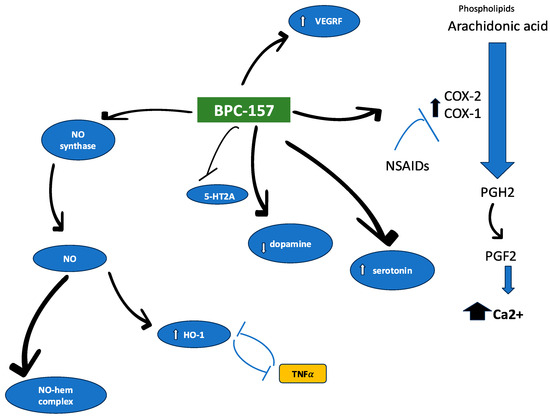
Product/visual context: what you might see in peptide research summaries
Many reviews include illustrative figures showing experimental outcomes or structural context. Here’s an example image commonly encountered in compiled scientific discussions:
Practical evaluation checklist for anyone assessing BPC 157 for gut conditions
If your goal is to form a grounded opinion about bpc 157 diverticulitis relevance, use this evidence checklist. It’s the same one I apply when I triage claims during research synthesis:
| What to check | Why it matters | What “good” looks like |
|---|---|---|
| Disease specificity | Different GI diseases can share inflammation but differ in drivers | Models that better resemble diverticulitis mechanisms and progression |
| Outcome endpoints | Molecular changes may not translate to clinical resolution | Resolution-related outcomes, complication-relevant markers, safety monitoring |
| Dosing/exposure alignment | Route and exposure determine where and how strongly effects occur | Pharmacology that supports plausible local exposure in the relevant tissue |
| Study design quality | Small or underpowered studies overestimate effect sizes | Replicates, clear controls, and adequate reporting |
| Patent scope realism | Patents can cover broad claims without proving clinical efficacy | Claims that match tested endpoints and supported data density |
Limitations you should not overlook
To keep this objective, here are the most important limitations that repeatedly appear in translational peptide narratives:
- Indication gap: multifunctional tissue-protection signals do not automatically establish diverticulitis treatment.
- Endpoint mismatch: many studies emphasize biomarkers or protective effects rather than clinically meaningful resolution outcomes.
- Human translation: GI inflammation in humans is heterogeneous, and disease severity timing affects what “benefit” means.
- Evidence hierarchy: patents can show intent or coverage, but they are not substitutes for controlled clinical evidence.
When I’ve seen these gaps, the most common failure mode is treating a plausible mechanism or preclinical protection result as if it were already validated for a specific acute condition like diverticulitis.
FAQ
Is there direct clinical evidence that BPC 157 treats diverticulitis?
Claims online often outpace clinical evidence. In evidence-based reviews, you should look specifically for well-designed human studies addressing diverticulitis outcomes. General GI protection data from preclinical work is not the same as demonstrated clinical efficacy for diverticulitis.
Why do people connect BPC 157 to gut inflammation in the first place?
Because reported preclinical effects often involve inflammation modulation and tissue-protection pathways, which are relevant to how GI injury can evolve. That connection is mechanistically plausible, but it remains a hypothesis until disease-specific outcomes are supported in humans.
What’s the most reliable way to judge whether “bpc 157 diverticulitis” is credible?
Use disease specificity, outcome endpoints, and exposure/route alignment as your primary filters. If the evidence is mostly indirect (generic inflammation models, biomarkers only, weak endpoint relevance), treat it as suggestive rather than actionable.
Conclusion: what to take away and what to do next
BPC 157 is frequently described as multifunctional because preclinical research suggests effects across inflammation and tissue protection pathways, including GI-related contexts. That is the underlying reason interest in bpc 157 diverticulitis emerges—but diverticulitis is clinically complex, and indirect evidence is not the same as validated treatment. The most trustworthy path is to evaluate disease specificity, clinically meaningful endpoints, and exposure alignment rather than relying on broad “gut healing” narratives.
Next step: If you’re reviewing any source making a diverticulitis claim, take the checklist above and score it against specificity, endpoints, study design, and patent scope realism before you consider the hypothesis credible.
Discussion